WE COULD HAVE SAVED THOUSANDS OF LIVES
Contributors: Dr. Sacoby Wilson, Sakereh Carter, and Aliyah Adegun
In an ideal world with a cohesive and competent COVID-19 response plan, the COVID-19 pandemic would have gone like this: Non-negotiable weekly testing across the nation, mandated proper personal protective equipment in public spaces, targeted interventions in low-wealth communities of color, stricter Environmental Protection Agency (EPA) industrial emission standards, livable monthly stipends for all citizens and non-citizens, eviction protection and rent forgiveness, and the proper allocation of resources to health care facilities. Instead, health care facilities are ill-equipped to handle the high volume of COVID-19 patients, people like Calvin Munerlyn are getting shot for asking a customer to put a piece of cloth around their cheeks [1], Blacks are more than twice as likely to die from COVID-19 [2] (See Table 1), the EPA ROLLED BACK pollution standards during the crisis [3], we’ve received ONE government-issued stipend check [4], 30–40 million people are at risk for eviction [5], and insufficient hospital infrastructure impedes high quality care across the nation [6].
This LACKADAISICAL, IRRESPONSIBLE, NON-SCIENTIFIC, AND IMMORAL way of handling the COVID-19 pandemic has cost 186,000 American lives which for the most part COULD have been avoided by addressing systemic inequities PRIOR to the global crisis and FASTER intervention at the beginning of the COVID-19 pandemic. We’ve robbed TOO MANY people of the opportunity to watch their grandchildren graduate from high school, to wake up next to their child, to get married, or to say goodbye to their deceased loved ones IT’S TIME to (1) address structured inequalities that allowed COVID-19 to ravage the nation, (2) handle the current COVID-19 crisis properly, and (3) prepare for future pandemics so that this NEVER HAPPENS AGAIN.

The nation has observed a striking disparity in COVID-19 morbidity and mortality rates between Whites and Black, Indigenous and People of Color since the beginning of the pandemic. In fact, Blacks, Latinx, and Native Americans are 2.2x, 1.1x, and 1.4x more likely to die from COVID-19 (See Table 1). As of April 15, 2020 Blacks comprise 30% of COVID-19 cases, even though they make up 13% of the total US population [7]. WHY? Pre-existing, social and environmental inequalities have EXACERBATED COVID-19 related ailments in low-wealth Black, Indigenous, and People of color (BIPOC) communities due to ineffective interventions, racist and opportunistic zoning and planning practices, devaluation of BIPOC communities, disinterested leadership, and inequitable distribution of power and resources.

As of May 19th, 2020, the state of Maryland ranked among the top 10 states with the highest COVID-19 cases and inadequate testing infrastructure [8]. As of September 3rd, 2020, Maryland state has reported 109,319 COVID cases and 3,623 deaths [9] (See Figure 1, 2). Within the state of Maryland, which counties are disproportionately impacted by COVID-19? On July 7th, 2020 Prince George’s County reported it’s 19,000th COVID-19 case surpassing the COVID-19 case number for 20 U.S. states combined [10]. Why? Prince George’s County is touted as “the country’s wealthiest majority-Black county”, but communities within the county experience chronic health conditions, food inequity, environmental hazards, and recently COVID-19 related ailments. Prince George’s County is 86% people of color and 9.8% of residents are designated low-wealth [11].

Characteristics of Prince George’s County that make its residents more susceptible to the global pandemic:
(1) HEALTH DISPARITIES: Prince George’s County ranks 14th among Maryland’s 24 counties for quality of community health [11]. Prince George’s County residents are disproportionately afflicted with chronic health conditions including heart disease, cancer, stroke, and diabetes. IN FACT, the rate of death from chronic related illness in the county is higher than all Maryland counties, the state, AND THE NATION [11]. One study found that people with chronic health conditions are TWELVE TIMES MORE LIKELY to die from COVID-19 [12]. What are the root causes of health inequity? According to Negussie et al., 2017, health inequities are attributed to racism, discrimination, residential segregation, food insecurity, lack of education, poor income and wealth, improper health systems and services, inadequate housing, insufficient parks and green space, climate change, poor transportation, the criminal justice system, police brutality, and overall public safety [13] (See Quote 1). As you can see, the entire lifestyle of BIPOC communities is TOXIC and multifactorial and must be treated as such.
(2) HEALTH CARE INFRASTRUCTURE: The ratio of primary care physicians to patients is 1,860:1 in Prince George’s County [11]. Thus, a county whose COVID-19 cases have skyrocketed has insufficient hospital infrastructure. The volume of COVID-19 patients in Prince George’s County is so high that many patients are transferred outside the county. Patients that arrive at Fort Washington Medical Center are often severely ill and doctors treat patients in surgical tents to keep up with the volume of patients [14]. How do you expect to receive high-quality health care with such a high ratio of patients to physicians? Healthcare infrastructure also entails providing residents with the proper personal protective equipment (PPE) to protect themselves from COVID-19 infection. Zenobia Shepherd, a Prince George’s County resident was unable to purchase respiratory masks at her local pharmacy, but easily identified face masks in Alexandria, VA [14].
(3) FOOD INSECURITY: Approximately, 71% of Prince George’s County residents are food insecure, meaning that most residents lack access to affordable, healthy food [11]. Food insecurity increases the risk of developing chronic health conditions including high blood pressure, coronary heart disease (CHD), hepatitis, stroke, cancer, arthritis, chronic obstructive pulmonary disease, and kidney disease [15]. Therefore, Prince George’s County residents are eating food devoid of any nutritional content and over time they’re developing chronic health conditions. When the COVID-19 pandemic struck Prince George’s County, these residents were designated high-risk populations because they harbor a chronic health condition that was created by racism and external forces that are OUTSIDE OF THEIR CONTROL.

(4) LEAD: Deterioration of lead paint from dilapidated housing units is the primary source of lead exposure in Prince George’s County [16]. Lead exposure has been shown to affect educational attainment and intellectual capability [17]. Prolonged exposure to lead is associated with an increased risk of chronic health conditions including high blood pressure, heart disease, and infertility [18]. Stay-at-home orders are not always the safest option for low-wealth communities of color, as they are forced to reside in toxic homes that are often inundated with lead, mold, and pests [19] (See Quote 2).
(5) OVERCROWDING: According to Prince George’s County City Council, 6,712 households in Prince George’s County are overcrowded [20]. Moreover, 85% of rented and 47% of owned homes are overcrowded [20]. A study conducted by Melamed et al., 2020 found that low socio-economic households and overcrowded residential housing units have a greater COVID-19 infection risk [21]. Not only are BIPOC households packed like sardines because they can’t afford to live COMFORTABLY, but they’re living conditions may cost them their lives.
(6) ESSENTIAL WORKERS: Prince George’s County has a high proportion of essential workers that sustain Maryland’s economy [22]. Specifically, Montgomery County and Prince George’s County make up 40% of the state’s economy [22]. Mack, a “44-year-old disease intervention specialist” and Prince George’s County resident lost her life to COVID-19 when the virus spread throughout the Prince George’s County Health Department [22]. Mack’s coworker exclaimed “We’re the ones called to the fire to do this during an emergency. We are essential. People don’t look at us as first responders, but we are [22].” Mack’s brother said, “She was a good soul- strong…It’s so messed up.” We have taken essential workers for granted and they DESERVE protection. Who do you think stocked the grocery shelves when we were ordered to stay-at-home? Who continued to deliver our packages? Who continued to pick up your trash, so that you could have clean streets every morning? Think about who REALLY MATTERS in this society and ask yourself if we’ve treated them with respect during this crisis [23] (See Quote 3).
“Many [Black and Brown people in the US] can’t afford to not work, or are on the front lines in jobs such as grocery clerks, janitors, or bus and train operators. Many rely on public transportation and are experiencing forced exposure. …Economics influences these decisions. It’s not about the body itself, but the societal situation in which the body is embedded [23].”
(7) MISTRUST OF MESSAGING: BIPOC populations are less likely to seek healthcare when necessary due to a history of medical malpractice, experimental exploitation, and capitalistic abuse. In the Tuskegee Syphilis Study, 400 African-American males were enrolled in a clinical trial from 1932–1972 to rectify “bad blood” [24]. In reality, the males were injected with syphilis to study the natural progression of the disease. Michael Brown, a barber and Prince George’s County resident exclaimed “Black residents understandably think, before you come in here to prick for my blood or ask for my DNA, I need to trust you [25].”
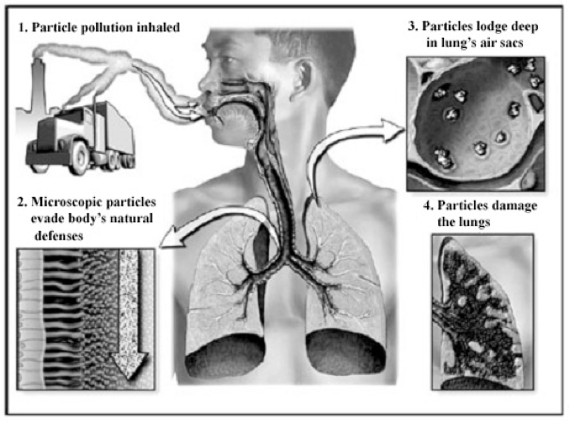
(8) ENVIRONMENTAL HAZARDS: Prince George’s County has a VERY high number of environmental hazards. The county hosts 14 Toxic Release Inventory (TRI) facilities, 6 brownfields, and 5 power plants [11]. THE GRADE FOR AIR QUALITY IN Prince George’s County IS AN F. The average Particulate Matter (Pm2.5) concentration in Prince George’s County is 9.9 ug/m3 relative to the national average of 6.7 ug/m3 [26]. Exposure to particulate matter is associated with cardiovascular disease, asthma, lung cancer, impaired immunity, and premature death [27] (See Figure 3).

In 2016, industries in the county emitted 23,827 pounds of toxic compounds into the air, water, and soil [28]. The majority of compounds released include sulfuric and hydrochloric acid, n-hexane, hydrogen fluoride, and ammonia [28] (See Image 1).
Recent studies have demonstrated that PM2.5 impairs immune function and enhances severe COVID-19 related outcomes [29]. Wu et al., 2020 investigated 3,000 U.S. counties and found that counties with high levels of PM2.5 have higher COVID-19 death rates relative to counties with lower PM2.5 levels [30]. FOLLOWING THE EPA-MANDATED ROLLBACK OF INDUSTRIAL EMISSION REPORTING, U.S. counties with higher TRI sites exhibited a 13% increase in pollution and a 38.8% increase in COVID-19 cases, respectively [31].
Protecting the environment is an ongoing process that has dire implications for BIPOC communities if not taken seriously. Economic circumstances should not dictate whether you have access to clean drinking water, air, and soil. Living in a clean environment is a fundamental right. It is unjust and irresponsible to place toxic facilities in BIPOC communities and abandon protective practices that preserve the health of humans and the environment. Our society has become so decadent that we allow rapacious corporations to poison human beings for capitalistic gain. “It depends on how society treats you — whether you need to go to the hospital or intensive care or need a ventilator,” said Dr. Stephen Thomas, the head of the Maryland Center for Health Equity at the University of Maryland [14].
Too much emphasis has been given to unfettered industrial and real estate development with limited to no focus on pollution prevention policies, and enforcement of and compliance with zoning regulations. Permits are now seen as a business market of exchange, giving freedom to industries to not be held accountable for the risks that they pose to the environment, public health, and quality of life.”- Dr. Sacoby Wilson [11].
Many of the COVID-19 related deaths in Prince George’s County are attributed to pervasive environmental injustices that were never addressed, suggesting that these losses were ENTIRELY PREVENTABLE. Specifically, if county leadership was more serious about environmental justice issues, we wouldn’t have observed stark disparities in COVID-19 related outcomes.
Brandywine, MD — In 2016, the Brandywine TB Coalition and Patuxent Riverkeeper filed a complaint against the Department of Transportation and the US EPA’s Office of Civil Rights regarding a proposed power plant operation [32]. The complaint raised concerns about adverse health effects associated with power plant operations that release particulate matter, nitric dioxide, and ozone precursors. If permitted, Brandywine would host a total of five power plants within a 13-mile radius [11]. Brandywine, MD is 72% black with a population of fewer than 7,000 people. Brandywine, MD residents suffer from various chronic health conditions that enhance the severity of COVID-19 including heart disease, asthma, stroke, emphysema, bronchitis, and chronic obstructive pulmonary disease [11]. “According to the Prince George’s County 2016 Community Health assessment, respiratory symptoms are the leading cause of emergency room visits in the County [33].” In Prince George’s county, Subregion 4 encompasses neighborhoods in Cedar Heights, Cheverly, and Fairmount Heights. Subregion 4 is 88% Black and hosts 35% of the county’s industrial facilities. According to the US EPA EJ screen, Subregion 4 is in the 95th percentile for particulate matter emissions [34].
CLEARLY, the Prince George’s County Council and County Executive underestimate the impact of zoning and planning ordinances and socio-environmental hazards on low-wealth BIPOC communities.
Council members of color also lack concern for EJ issues in Prince George’s County. Environmental classism is “the process by which economically disadvantaged and undereducated populations are disparately burdened by environmental hazards, particularly unwanted land uses (LULUs).” Typically, environmental racism and classism go hand-in-hand; but; sometimes classism transcends race. A public health official stated that environmental injustice cannot occur in Prince George’s County because Prince George’s County leadership is majority black [11]. This sentiment implies that Blacks cannot inflict harm on other blacks. In reality, the “I scratch your back and you scratch mine” dynamic between political leaders and lobbyists perpetuates the discriminatory siting of toxic facilities in BIPOC communities [35].
“Economic Matters Chairman Dereck E. Davis (D-Prince George’s) is the sponsor of a local bill that would repeal the prohibition on developers or their agents making campaign contributions to the Prince George’s County executive or a political slate that includes the county executive when the developer has a proposed project pending before the county government [35].”
Prince George’s County Environmental Justice Commission (HB1362) published a detailed report in 2020 that prioritizes how to address environmental injustice in Prince George’s County [34]. The plan of action includes:
(1) Green and healthy zoning and planning practices that protect communities from disparate concentrations of polluting entities, (2) cumulative impact assessments, (3) the creation of environmental benefit districts (EBDs), and (4) meaningful community engagement. Recommendation #1 aims to address inequitable zoning and planning decisions by using the Maryland EJ screen tool to identify EJ communities, require permit applicants to provide regional environmental quality data (air, soil, and water) for all proposed operations, and allow for the County Council to enforce stricter regulations to protect the health of BIPOC communities. If implemented, the plan would require community input when drafting Health Impact Assessments (HIA) which is usually bypassed due to a 30-day grace period following receipt of an M-NCPPC. Recommendation #2 seeks to reduce the cumulative burden in BIPOC communities by discouraging the aggregation of industrial operations. Currently, the planning department “does not have a mechanism for prohibiting saturation of specific or brands of used during the development process. Recommendation #3 aims to increase the amount of health-promoting infrastructure in EJ communities. Recommendation #4 highlights the importance of community involvement and explicit instructions for meaningful community engagement in ALL environmentally-related plans, decisions, and enforcement.
WHAT STEPS HAS THE PRINCE GEORGE’S COUNTY COUNCIL MADE TO IMPLEMENT THE RECOMMENDATIONS DETAILED in the Prince George’s County Environmental Justice Commission (HB1362) report & The University of Maryland Environmental Justice Plan 2025? The county lacks a strong plan for COVID-19 mitigation, elimination of health disparities, and reduction of environmental hazards. WE ARE IN A SYNDEMIC. A syndemic is “two or more afflictions, interacting synergistically, contributing to an excess burden of disease in a population” [36]. TOXIC POLLUTION, RACISM, ECONOMIC DISPARITIES, AND COVID-19 IS KILLING BIPOC AND IT’S OUR MORAL OBLIGATION TO ELIMINATE ALL FORMS OF INJUSTICE IN AMERICA. When everything is said and done, which side of history do you want to be on?
References
- https://www.bbc.com/news/world-us-canada-52540266#:~:text=Calvin%20Munerlyn%2C%2043%2C%20was%20shot,without%20a%20state%2Dmandated%20mask.
- https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html
- https://www.nytimes.com/2020/03/26/climate/epa-coronavirus-pollution-rules.html
- https://www.marketwatch.com/story/americans-need-more-than-a-1200-check-a-guaranteed-basic-income-is-the-stimulus-we-deserve-2020-04-27
- https://www.aspeninstitute.org/blog-posts/the-covid-19-eviction-crisis-an-estimated-30-40-million-people-in-america-are-at-risk/
- https://www.vox.com/policy-and-politics/2020/3/16/21173766/coronavirus-covid-19-us-cases-health-care-system
- https://www.samhsa.gov/sites/default/files/covid19-behavioral-health-disparities-black-latino-communities.pdf
- https://scotteblog.com/2020/05/19/maryland-ranks-in-the-top-10-for-covid-19-cases-and-deaths-trails-many-states-in-testing/
- https://coronavirus.maryland.gov/
- https://www.wusa9.com/article/news/health/coronavirus/prince-georges-county-has-had-more-coronavirus-covid19-cases-than-20-states/65-f3e9e0c4-65d1-4b8c-bebd-f218aca10470
- http://www.btbcoalition.org/index%20page%20images/ENVIRONMENTAL%20JUSTICE%20PLAN%202025_PrinceGeorges.pdf
- https://medicalxpress.com/news/2020-06-covid-death-higher-chronic-health.html
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on Community-Based Solutions to Promote Health Equity in the United States; Baciu A, Negussie Y, Geller A, et al., editors. Communities in Action: Pathways to Health Equity. Washington (DC): National Academies Press (US); 2017 Jan 11. 3, The Root Causes of Health Inequity. Available from: https://www.ncbi.nlm.nih.gov/books/NBK425845/; https://www.baltimoresun.com/coronavirus/bs-md-prince-georges-coronavirus-20200709-pawnopbtgngx7kh6cmq6ugldni-story.html
- https://www.washingtonpost.com/local/prince-georges-maryland-coronavirus-health-disparities/2020/04/26/0f120788-82f9-11ea-ae26-989cfce1c7c7_story.html
- https://www.minnpost.com/second-opinion/2017/08/food-insecurity-linked-10-major-chronic-diseases/#:~:text=It%20found%20that%20low%20food,(hypertension)%2C%20coronary%20heart%20disease
- https://www.baltimoresun.com/news/investigations/bs-md-lead-poisoning-react-20151207-story.html
- https://digitalcommons.otterbein.edu/stu_msn/111/
- https://www.cdc.gov/niosh/topics/lead/health.html
- https://frankellawfirm.com/lead-poisoning-dangers-lurk-in-the-shadow-of-covid-19/
- https://www.princegeorgescountymd.gov/DocumentCenter/View/4076/Prince-Georges-County-Draft-Consolidated-Plan-2016---2020-PDF?bidId=
- Columbia University Irving Medical Center. (2020, June 18). Crowded homes, poor neighborhoods linked to COVID-19. ScienceDaily. Retrieved September 8, 2020 from www.sciencedaily.com/releases/2020/06/200618124756.htm
- https://khn.org/news/essential-and-in-danger-coronavirus-sickens-even-kills-public-health-workers/
- https://www.fr24news.com/a/2020/04/why-the-coronavirus-is-ravaging-prince-georges-county-a-rich-black-county-in-maryland.html ;https://ihpi.umich.edu/news/racial-disparities-time-covid-19
- https://www.history.com/news/the-infamous-40-year-tuskegee-study
- https://www.baltimoresun.com/coronavirus/bs-md-prince-georges-coronavirus-20200709-pawnopbtgngx7kh6cmq6ugldni-story.html
- https://www.epa.gov/ejscreen
- Lee, K. K., Miller, M. R., & Shah, A. (2018). Air Pollution and Stroke. Journal of stroke, 20(1), 2–11. https://doi.org/10.5853/jos.2017.02894; Hamanaka, R. B., & Mutlu, G. M. (2018). Particulate Matter Air Pollution: Effects on the Cardiovascular System. Frontiers in endocrinology, 9, 680. https://doi.org/10.3389/fendo.2018.00680; https://www.nih.gov/news-events/nih-research-matters/air-pollution-linked-risk-premature-death; Loxham, M., & Nieuwenhuijsen, M. J. (2019). Health effects of particulate matter air pollution in underground railway systems — a critical review of the evidence. Particle and fibre toxicology, 16(1), 12. https://doi.org/10.1186/s12989-019-0296-2; https://www.ecowatch.com/u-s-epa-sued-for-failure-to-issue-air-pollution-standards-1881589230.html
- US EPA. (2016, March). TRI Explorer. Retrieved 2018, from https://iaspub.epa.gov/triexplorer/release_chem?p_view=COCH&trilib=TRIQ1&sort =_VIEW_&sort_fmt=1&state=24&county=24033&chemical=All%2Bchemicals&industry= ALL&year=2016&tab_rpt=1&fld=TSFDSP; https://apnews.com/cf311ecc8b054fa99c95a59d8eb45de1
- Comunian, S., Dongo, D., Milani, C., & Palestini, P. (2020). Air Pollution and Covid-19: The Role of Particulate Matter in the Spread and Increase of Covid-19’s Morbidity and Mortality. International journal of environmental research and public health, 17(12), 4487. https://doi.org/10.3390/ijerph17124487
- https://www.medrxiv.org/content/10.1101/2020.04.05.20054502v2
- Persico, Claudia and Johnson, Kathryn R., The Effects of Increased Pollution on COVID-19 Cases and Deaths (June 22, 2020). Available at SSRN: https://ssrn.com/abstract=3633446
- Blackner, E. (2016). Fighting food deserts a collaborative effort — Prince George’s Sentinel. Retrieved March 2, 2018, from http://www.thesentinel.com/pgs/index.php?option=com_k2&view=item&id=3218:fighting -food-deserts-a-collaborative-effort&Itemid=766
- https://pophealth.health.maryland.gov/Documents/Resources/Prince%20George%27s_CHNA_2016.pdf
- https://msa.maryland.gov/megafile/msa/speccol/sc5300/sc5339/000113/024500/024590/20200376e.pdf
- https://www.marylandmatters.org/2019/01/24/prince-georges-lawmakers-ponder-bill-to-unleash-developer-cash/
- Wilson, P. A., Nanin, J., Amesty, S., Wallace, S., Cherenack, E. M., & Fullilove, R. (2014). Using syndemic theory to understand vulnerability to HIV infection among Black and Latino men in New York City. Journal of urban health : bulletin of the New York Academy of Medicine, 91(5), 983–998. https://doi.org/10.1007/s11524-014-9895-2
